


Lp(a) – the other lipoprotein you don’t hear about much ...
Unveiling Lp(a): The Silent Threat to Heart Health Beyond LDL Cholesterol. Guest post by Suri (Narayanan Surendran, Pharma scientist)

“In Sicily, women are more dangerous than shotguns” is likely to be in top 10 of quotes from The Godfather; at least for some readers of this article. It is generally thought that this stems from the protective instincts of fathers (with shotguns, naturally) who may be concerned about their daughters’ welfare. However, that is not entirely true. Much as we “admire” the men in gangster movies, it turns out the “gentler and kinder” variety of our species can also be ruthless as perpetrators as they are victims of crime.
Now that I have your attention, you may be asking what does it have to do with Lp(a)? Well, the short answer is while LDL (low density lipoprotein i.e., “bad cholesterol”) has been hogging the headlines for over four or five decades now, the shy, reticent version that is Lp(a) has not only completed it’s debutante ball in stunning glory in recent years (albeit in scientific conferences), it is ready for prime time. By the way, Lp(a) is typically pronounced as “el pee little a”.
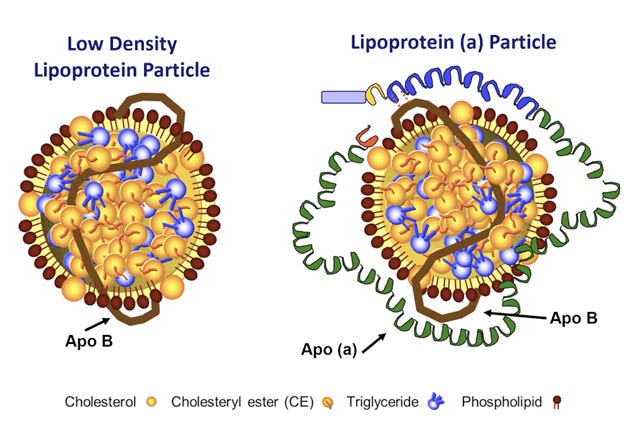
Some basics first – Lp(a) is a lipoprotein that has Apo B similar to LDL but is tethered to another apolipoprotein called Apo(a) and it is the latter that defines Lp(a)’s distinct personality. Apo(a) is produced in the liver and interacts with fibrinogen, a molecule responsible for clotting; one reason why it leads to certain pathologies associated with elevated Lp(a). Now, the question is why should we be bothered by this nastier cousin of LDL? Turns out while the existence of Lp(a) has been known for some time, over the last decade or so, researchers have learned a lot more about it and we now have enough evidence to suggest this should not be overlooked, at least in certain high risk patients.
For starters, we now have epidemiological and genetic information to suggest Lp(a) is causally related to atherosclerotic cardiovascular disease (ASCVD). In addition, thanks to its fibrinogen binding domain, it can also cause thrombosis and finally, it also contributes to aortic valve calcification. In other words, even if LDL, the big brother, has been somewhat tamed now, we now understand enough about Lp(a) that makes it awfully hard to ignore it. Much like other ‘biomarkers’ of health, researchers have studied various components of Lp(a) production, assembly, and concentrations in plasma. One aspect that really stands out with Lp(a) is that about 70 to 90% of its plasma levels are genetically determined (other factors being medical conditions and environment) so the age-old advice that we should choose our parents carefully applies to this as well! If you have read this far along and know what you know now, you may be tempted to declare “Ha, I will get my levels tested ASAP and hit them with some drugs so what’s the big deal?”.
Well, like most things in life, point A to point B is usually not a straight line and turns out it is no different for Lp(a). Since a good amount of it is genetically determined and comorbidities are likely to influence plasma levels, we don’t have a good sense (or as good as it is for LDL with warts and all) to help define universal thresholds that we can use clinically to assess risk for any particular individual. So, given this scenario, what is one to do right today? One obvious item on the To Do list is to add Lp(a) to the blood panel at your next regular (annual) check-up. While it is important for folks with high risk of ASCVD to learn about their Lp(a) status, it may still be useful to get this test done once even if your 10 year risk for ASCVD is low - reason being, a full understanding of Lp(a)’s role in other pathophysiology (i.e., other than ASCVD) is still unclear. Don’t be surprised if your physician is not aware of Lp(a) in any detail – that is what happened to me during my check up in 2021 and fortunately for me, when I explained why I would like to get it tested (to establish my broad risk category), he did not hesitate to add it to the list. Our current data for reference range for Lp(a) is that less than 30 mg/dL is considered to be in the normal range (mine was 21 mg/dL). Of course, this brings up the question, what if yours is > 30 mg/dL? Recall, I mentioned earlier, we still do not have a good sense for how to set thresholds – that is still somewhat true and until we have drugs that have been launched and clinical outcomes data becomes available, there is not much within our agency at this time with regard to drug intervention for reducing plasma levels of Lp(a).
However, what is still useful in my opinion is to educate ourselves a bit more about it and also assess how elevated Lp(a) may reclassify your risk for ASCVD beyond what we now do with LDL levels (and other risk factors). Luckily for us, the American Heart Association released a consensus statement in 2022 on this specific topic. I will direct your attention to Table 5 of this statement that speaks to how to evaluate risk based on your Lp(a) plasma levels. Briefly, it advises us to use 10 year risk (pooled cohort equation or some other validated tool) for CV risk and update with Lp(a) information you obtain from your blood test.
Now, since Lp(a) levels are largely genetically determined, you will not need to test it regularly – one time testing to understand where you fall in the risk category should be adequate – after all, to be forewarned is to be forearmed.
Meanwhile, if you have been conscientious about your CV health and have already embraced good behaviors regarding diet, exercise, sleep etc., continue to do so! OTOH, if you are still struggling with incorporating the above and if your Lp(a) levels are > 30 mg/dL, you have just discovered another risk factor for ASCVD – all the more reason you will need to seriously consider lifestyle change(s) to reduce your overall risk of cardiovascular disease – both morbidity and sadly, mortality.
Takeaway: If you have not had your Lp(a) levels measured in the past, now would be a good time to get it measured so you can understand your potential risk. Since it is genetically determined, you may also want to encourage your siblings (if any) to get tested. Although this information is not currently actionable, if your levels are >30 mg/dL, you should talk to your physician at some point close to the launch of drugs being developed now to figure out if you may be a good candidate for this therapy (in future).
 | A guest post by
|