


CCTA - Early Detection Tool for Cardiovascular Disease
Coronary CT angiography (CCTA) is emerging as a powerful, non-invasive tool for early detection of heart disease

Every year, countless families grapple with the anguish of losing loved ones to heart attacks, often occurring suddenly while engaged in everyday activities such as playing sports or carrying out routine tasks. A 2021 report by the American Heart Association suggests that "silent" heart attacks may account for over 20-45% of the approximately 850,000 heart attacks that occur in the United States every year. Moreover, nearly 80 percent of heart attacks in the US go undiagnosed, which includes those that are silent1 and not recognized at the time they occur. These statistics imply that a substantial number of heart attacks, including those that might lead to hospital admissions, could occur without symptoms. Silent heart attacks elevate the risk of future heart attacks, as even minor ones can result in tissue scarring and further damage to the heart muscles.
This is one of the reasons I strongly recommended that everyone undergo a Calcium CT scan to proactively detect plaques in the coronary arteries, which are indicative of cardiovascular disease. A Calcium CT scan provides information about plaque burden, unlike a stress test, which can only identify significant blockages of 70% or more in the coronary arteries. However, the majority of heart attacks stem from the rupture of plaques causing less than 50% narrowing. The results of stress tests can sometimes be misleading, indicating coronary artery disease in people who do not actually have the condition, or missing it in those who do. A negative stress test does not entirely eliminate the presence of plaque.Moreover, stress tests are aimed at detecting reduced blood flow due to severe blockages and cannot directly visualize arterial plaque buildup. They offer functional insights but lack anatomical detail regarding plaque. Unfortunately, stress test continues to be the current standard of care for patients who complain of chest pains (angina)
Although a Calcium CT scan serves as a valuable first step and may lead your clinician to initiate statin therapy in case of a high score, it's important to note that it can only detect calcified plaques. On the other hand, Coronary Computed Tomography Angiography (CCTA) with contrast can detect both calcified plaques and low-density non-calcified plaquesin the coronary arteries. CCTA is a noninvasive diagnostic imaging test that uses a combination of X-rays and computing to produce detailed 3D images of the coronary arteries. CCTA is used to identify plaque buildup and blockages or narrowing (stenosis) in the coronary arteries. During a CCTA procedure, a contrast dye is injected through an intravenous (IV) line to make the coronary arteries visible on the images.
Calcified vs. Non-calcified (soft) plaques
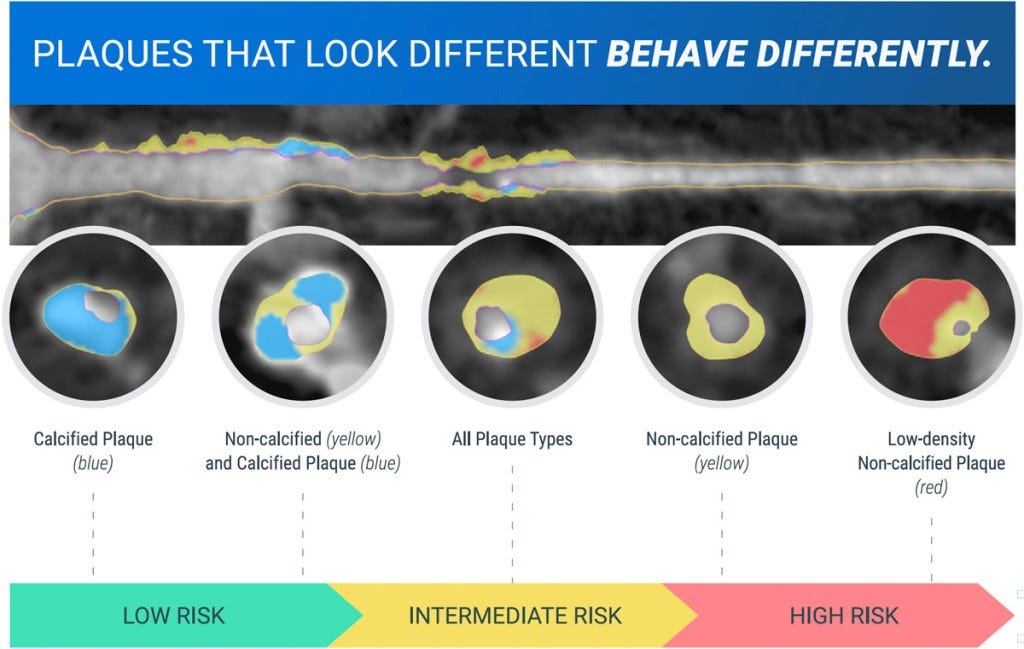
The image depicts various types of plaques alongside their corresponding risk levels. Calcified plaques contain significant amounts of calcium deposits. The presence of calcified plaque is a clinical marker of cardiovascular diseases and indicates the buildup of fatty deposits, cholesterol, calcium and other substances in the artery wall over time. Calcified plaques are more stable and less likely to rupture compared to non-calcified (also called soft) plaques. However, they can still cause narrowing of the artery. Non-calcified plaques, also known as soft plaques contain little to no calcium deposits. Non-calcified plaques are composed primarily of lipids (fatty deposits), inflammatory cells, and connective (fibrous) tissue, making them soft and unstable. This instability means that soft plaques can rupture suddenly, leading to the formation of blood clots that can block blood flow to the heart or other vital organs. They lack the dense calcium deposits that define calcified plaques. Non-calcified plaques represent an earlier stage of cardiovascular disease compared to calcified plaques. Moreover, these plaques are typically lipid-rich and exhibit lower density on CCTAs compared to calcified plaques. This contrast enables them to be differentiated from the denser and more stable calcified plaques. Plaque calcification is a late manifestation, so the presence of non-calcified plaque indicates that the disease is still in its initial stages. While calcified plaques are associated with a higher overall plaque burden, recent research suggests soft plaques may be more predictive of adverse cardiovascular events like heart attacks. Additionally, soft plaque is associated with an increased risk of aneurysms, which are potentially life-threatening bulges in blood vessel walls. Several studies have found evidence of early atherosclerosis and plaque formation in the coronary arteries of young individuals. According to the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study, which investigated 2,876 people aged 15-34 who died from accidents, homicides or suicides, fatty streaks and early plaques were already present in the aorta and coronary arteries of many teenagers and young adults. Another study comparing plaque characteristics in young adults (mean age 27) versus older adults (mean age 58) with symptomatic intracranial atherosclerotic stenosis found that early plaque development was significantly more common in the younger group.
CCTA can detect both soft, non-calcified plaques and calcified plaques in the coronary arteries. Thus, CCTA can provide information on overall plaque composition, while a Calcium CT scan provide a score based on the amount of calcium. CCTA has high sensitivity (87%) and specificity (98%) for detecting non-calcified plaques when compared to the gold standard of optical coherence tomography (OCT), which is an invasive procedure performed in the catheter-lab. CCTA allows for visualization of the entire coronary tree: knowledge of the location and extent of plaques is important for risk assessment and treatment planning. As CCTAs can identify non-calcified plaques, an early sign of cardiovascular disease, there's growing support for its utilization as an early detection method.
While a CCTA is not very expensive (costs between $311 to $737 on average), it is typically prescribed by a cardiologist only when the patient presents with symptoms such as chest pain. This review suggests that CCTA is a cost-effective strategy for low risk patients presenting to the emergency department (ED) with acute chest pain. In such patients, CCTA provides a cost-effective diagnostic strategy with the potential to reduce economic burden and improve long-term health outcomes. However, some patients may experience allergic reactions from the iodine-containing contrast material used during the procedure. Radiation exposure and the potential for downstream unnecessary invasive angiography procedures are additional downsides.
The emergence of CCTA along with artificial intelligence (AI) is showing great promise as an early diagnostic tool for cardiovascular disease. CCTA provides high-resolution images of the coronary arteries, allowing for the detection of both calcified and non-calcified plaques. However, interpreting these images can be time-consuming and prone to errors, especially with the increasing demand for CCTA examinations. AI has the potential to revolutionize the field of cardiac imaging by automating various aspects of the CCTA workflow, from image acquisition to plaque quantification and risk assessment. Numerous companies and startups currently offer AI-powered tools for CCTA analysis. Among them are Cleerly, Caristo Diagnostics, Elucid and Siemens Healthineers. Stay tuned for future posts where I'll explore each of them in more detail.
They are described as "silent" because when they occur, their symptoms lack the intensity of a classic heart attack, such as extreme chest pain and pressure; stabbing pain in the arm, neck, or jaw; sudden shortness of breath; sweating, and dizziness.