


Why LDL Particle Count and Size Matter More Than You Think
Traditional cholesterol tests can be misleading—understanding LDL particle size and count provides a clearer picture of cardiovascular riskLDL Particle Size

In a previous post on regular biomarker testing, I shared that my LDL-C was a solid 63 mg/dL—a number that would typically be considered reassuring based on a standard blood panel, where LDL-C is the primary focus. However, a deeper analysis of my LDL profile, provided by Function Health, painted a different picture. My LDL Particle (LDL-P) count came in at 1,368, exceeding the guideline of 1,138, making the results less reassuring. It turns out that the more LDL particles you have, the greater your risk of atherosclerosis. The figure below illustrates this concept clearly: two patients may have the same LDL-C level (130 mg/dL), but the patient on the right (Pattern B) has a higher LDL-P count, putting them at greater risk for cardiac events.

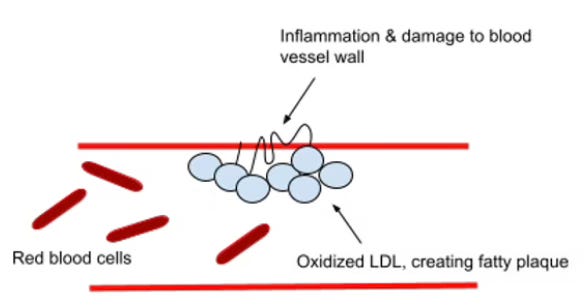
LDL-P count and particle size have emerged as a crucial metric for diagnosing cardiovascular disease risk, offering insights beyond traditional cholesterol measurements. Smaller LDL particles are associated with a higher risk of coronary artery disease (CAD) compared to larger particles. This is because smaller LDL particles are more likely to penetrate the arterial wall and become oxidized1, initiating the process of atherosclerosis. This relationship is significant in understanding cardiovascular disease risk and progression. Smaller LDL particles can more easily penetrate the arterial wall. This increased ability to enter the subendothelial space is a key factor in plaque formation. The smaller size allows these particles to slip through the gaps between endothelial cells more readily, initiating the atherosclerotic process. Once inside the arterial wall, smaller LDL particles are more likely to become trapped. They have a higher affinity for arterial proteoglycans2, which causes them to be retained within the vessel wall for longer periods. This prolonged retention increases the likelihood of oxidation and subsequent inflammatory responses, as shown in the figure below. Oxidized LDL plays a key role in atherosclerosis by triggering inflammation, which attracts monocytes3 to the affected area. These monocytes then transform into macrophages4 that engulf oxidized LDL particles, forming the early lesions characteristic of atherosclerosis.
In fact, the total number of LDL particles (LDL-P) has been shown to be a stronger predictor of cardiovascular disease (CVD) risk, then LDL-C or non-HDL-C measurements. For instance, the Framingham Offspring Study, a large community-based study found that LDL-P was more strongly related to future CVD than LDL-C or non-HDL-C in both men and women. Subjects with a low LDL-P (<25th percentile) had a lower CVD event rate (59 events per 1000 person-years) compared to those with equivalently low LDL-C or non-HDL-C (81 and 74 events per 1000 person-years, respectively).
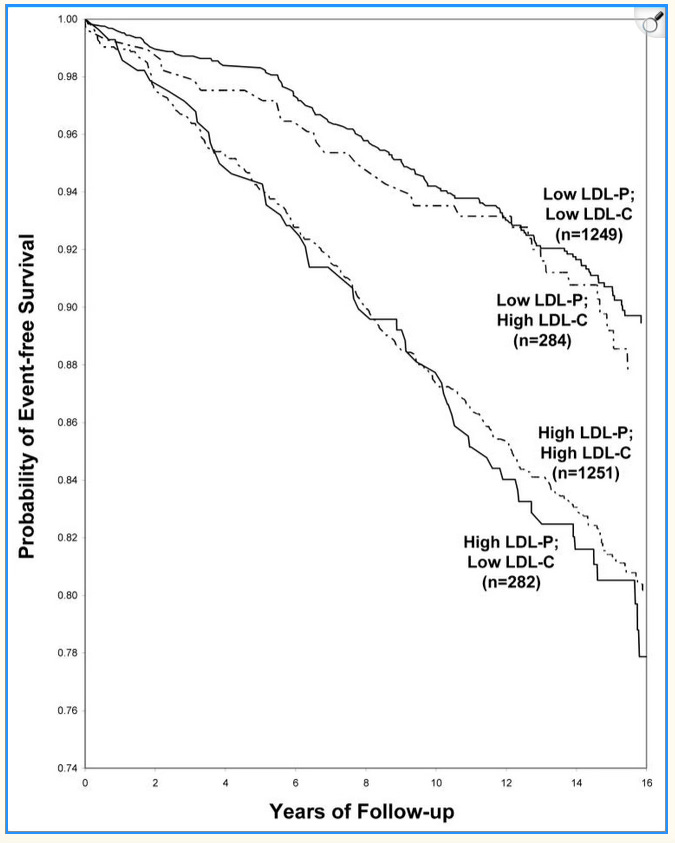
Event-free survival curves for participants with LDL-C and LDL-P levels greater or less than the median are shown in the accompanying figure. Event-free survival was clearly worse for individuals with low LDL-C and high LDL-P than for the group with high LDL-C and low LDL-P. Differences in LDL-C had little effect on event-free survival within both the high LDL-P and low LDL-P participants, signifying that LDL-P is the better predictor of CVD risk.
Furthermore, the composition of plaques formed by smaller LDL particles tends to be different from those formed by larger particles. Plaques with a higher proportion of small, dense LDL are often more vulnerable to rupture. This instability increases the risk of acute cardiovascular events such as heart attacks and strokes.
Clinically, several strategies can be employed to achieve a more favorable LDL particle size profile. Multiple studies have shown that statins can reduce LDL-P counts. A systematic review of 36 studies found that statins generally lowered LDL-P, though often to a lesser extent than they lowered LDL cholesterol (LDL-C). The fact that statins appear to be more effective at reducing LDL-C than LDL-P may explain some of the residual cardiovascular risk in patients who achieve LDL-C goals but still have elevated LDL-P. PCSK9 inhibitors have also shown ability to reduce LDL-P. A study on alirocumab, a PCSK9 inhibitor, demonstrated that it decreased LDL-P concentration across all subclasses, including a 71.3% reduction in large LDL-P and significant reductions in small LDL-P. Diet also plays a crucial role, with low-carbohydrate and Mediterranean-style diets showing promise in increasing LDL particle size. A randomized, crossover, controlled feeding trial demonstrated that including one avocado per day as part of a moderate-fat, cholesterol-lowering diet significantly decreased LDL-P. The avocado diet reduced LDL-P by 80.1 nmol/L from baseline. It also decreased small dense LDL (sdLDL), cholesterol by 4.1 mg/dL. These reductions were greater than those achieved by a moderate-fat diet without avocados or a lower-fat diet. Studies also suggest fruit consumption can help reduce small, dense LDL (sdLDL) particles. A review of seven studies found that six showed a significant reduction in sdLDL, while two out of four studies reported an increase in LDL particle size.
Regular exercise, particularly aerobic activities, has also been associated with improvements in LDL particle size. For instance, the Oslo Diet and Exercise Study, a 1-year randomized trial of 188 healthy middle-aged men, found that exercise significantly decreased apolipoprotein B (apoB) levels by 7.4% compared to the control group. ApoB is a surrogate marker for LDL-P, as each LDL particle contains one apoB molecule. This study provides strong evidence that exercise can reduce LDL-P. Losing even 5-10 pounds can improve your cholesterol profile and reduce small LDL particles. A study on overweight men found that a 20-pound weight loss significantly shifted LDL particle size and distribution. Among 15 men with small, dense LDL (Pattern B), 11 showed an increase in LDL peak particle diameter, with seven transitioning to an intermediate pattern and four shifting to the larger LDL particle pattern (Pattern A).
Takeaway: Traditional cholesterol tests focusing on LDL-C may overlook important risk factors for cardiovascular disease. LDL particle count (LDL-P) and particle size are more accurate predictors, as smaller, denser particles are more likely to penetrate artery walls, become oxidized, and contribute to plaque formation. Studies confirm that high LDL-P levels correlate with increased heart disease risk, regardless of LDL-C levels. Strategies like statins, PCSK9 inhibitors, dietary changes, exercise, and weight loss can help lower LDL-P and improve heart health outcomes.
In the context of atherosclerosis, "oxidized" refers to the chemical modification of LDL-C by reactive oxygen species (ROS).
A type of protein-carbohydrate complex (glycoproteins) found in the arterial wall, playing a crucial role in vascular function and disease, including atherosclerosis.
Monocytes are a type of white blood cell that play a crucial role in the immune system.
A type of white blood cell that surrounds and kills microorganisms, removes dead cells, and stimulates the action of other immune system cells.
Great post, Ram. I couldn't agree more that LDL-P and ApoB should be the gold standard.
It's frustrating that this thinking is still considered "advanced" when it has such critical real-world implications. My own experience with doctors dismissing a high ApoB reading is what led me to dive deeper into this topic and write about a framework for navigating it: https://mettaquant.substack.com/p/personal-preventive-medicine-part-1
Ram-so I have been writing about this for years. I’m on the editorial board of the journal of clinical lipidology, and a board-certified cardiothoracic surgeon. I also wrote Lipoprotein and Lipoprotein disorders: Current Clinical Guidelines with Tom Dayspring and Bill Cromwell. I am happy you wrote about this, but you need to correct the part about particle size. It does not matter and that has been to fitly shown. The size of a pore in the intima is 70nm and every ApoB with the exception of the largest chylomicrons get through the intimal wall, if present in high concentrations, I’ve written extensively about this on Substack